


































The PM’s call to cut cooking oil touches a structural problem with documented history, a mounting import bill, serious peer-reviewed health consequences — and evidence-based solutions that go well beyond a political appeal.

The Appeal and What Lies Behind It
When Prime Minister Modi, speaking in Hyderabad last month, called on Indians to reduce their consumption of cooking oil — alongside petrol, diesel, and gold — the appeal was prompted by immediate economic pressure. India imported 16 million tonnes of edible oils in 2024-25 at a cost of approximately Rs 1.61 lakh crore — the country’s third-largest import by value after crude petroleum and gold. With the West Asia conflict straining global supply chains and the rupee under pressure, the PM’s concern is economically well-founded.
But the problems the PM’s appeal touches are far older than this crisis. Why does India import the majority of its edible oil from Indonesia, Malaysia, Argentina, Brazil, and the former Soviet republics? Why has domestic production chronically fallen short?
And what does the peer-reviewed medical literature say about a consumption level now nearly double the ceiling recommended by India’s own Council of Medical Research? The answers — and the solutions — require a look at culinary history, agricultural economics, trade policy, and nutritional science.
Why Indian Cuisine Is So Heavily Fried
Ghee, Heat, and the Logic of a Pre-Refrigeration Kitchen
Few culinary traditions rely on oil as structurally as India’s. Parathas, puris, pakoras, samosas, bhajias — frying is not an occasional technique but a foundational one, embedded in daily eating across every region and income level.
The paratha — from the Sanskrit parat (layers) and atta (flour) — is among the oldest preparations in the North Indian culinary record. Its defining feature is the folding of ghee into wheat dough to create flaky layers. Ghee’s low moisture content and high smoke point made it the practical fat of a subtropical kitchen without refrigeration: it preserved, flavoured, and extended the shelf life of cooked food simultaneously.
Deep frying served similar practical ends. Food cooked in hot oil develops a sealed exterior that slows bacterial growth critically before cold storage existed. Regional oilseed surpluses provided the raw material: groundnut in Gujarat and Andhra Pradesh, mustard in Bengal and Bihar, sesame in Rajasthan, coconut along the coastlines. Frying at scale was fast and reliable for feeding large gatherings at festivals and weddings.
The Samosa: A Deep-Fried Import That Became Native
The samosa’s route to India is well documented. Its Persian ancestor, the sanbosag, appears in 10th-century Arab and Persian cookbooks. It reached India via the Delhi Sultanate in the 13th and 14th centuries: the poet Amir Khusro (c.1300 CE) recorded that Delhi court nobles enjoyed the “samosa prepared from meat, ghee, onion,” and the 14th-century Moroccan traveller Ibn Battuta described it at the Tughlak court.
By the 15th and 16th centuries it appears in Indian cookbooks including the Nimatnama-i-Nasiruddin-Shahi and the Ain-e-Akbari. Unlike its baked or pan-fried Middle Eastern counterparts, the Indian samosa became deep-fried — crispier, more shelf-stable, and better suited to street commerce.
The 20th-century replacement of ghee with cheap
refined palm oil was driven by economics, not tradition.
That single substitution lies at the heart of both India's
import bill and the health consequences documented below.
Why India Cannot Produce Enough?
India is simultaneously the world’s largest importer of edible oils and among its largest producers of oilseeds — a paradox at the heart of agricultural policy. Groundnuts, rapeseed-mustard, soybean, sunflower, sesame, and linseed cover approximately 13 per cent of the gross cropped area, yet domestic production meets only 40 to 44 per cent of national edible oil demand. The remaining 56 to 60 per cent is imported from geopolitically exposed supply chains.
A 2024 NITI Aayog report identified the structural causes: oilseed yields remain below global averages due to rain-fed vulnerability and deficient agronomic practice; landholdings are small and fragmented; and cheap imported palm oil has consistently undercut domestic prices, discouraging farmers from expanding cultivation.
India’s WTO commitments through the 1990s required reduction of import duties and withdrawal of price support, allowing Southeast Asian palm oil to displace domestic producers on price. Import dependence rose from approximately 15 per cent in 1995-96 to over 63 per cent by 2015-16, per Solvent Extractors’ Association of India (SEA) data, before easing modestly to around 56 per cent in 2023-24.
Edible oil is India's third-largest import after crude and
gold. In twenty years, the import bill grew 15-fold while
import volume grew only 2.2 times — a measure
of deepening structural dependence on
globally volatile commodity markets.
The government has acknowledged the failure. The National Mission on Edible Oils – Oilseeds (NMEO-OS), approved in October 2024 with a Rs 10,103 crore budget over seven years, targets an increase in primary oilseed production from 39 million tonnes in 2022-23 to 69.7 million tonnes by 2030-31. A parallel oil palm mission offers price guarantees to cultivators — palm yields approximately 14.6 tonnes of oil per hectare, far exceeding any other crop India grows at scale.
The Numbers: Scale and Exposure
India’s per capita edible oil consumption has risen from approximately 2.9 kg per year in the 1950s to 8.2 kg in 2001 and an estimated 23.5 kg in 2024-25, per SEA and NITI Aayog figures reported by Business Standard in April 2025. Total annual consumption stands at 25 to 26 million tonnes against domestic production of 9.6 to 11 million tonnes, leaving an import requirement of 16 to 17 million tonnes.
Palm oil alone accounts for over 37 per cent of total consumption. The demand surge has been driven by rising incomes, urbanisation, processed food growth, and the rapid expansion of the HoReCa sector — hotels, restaurants, and catering.
The NITI Aayog’s own modelling shows that if Indian consumers followed ICMR-NIN dietary guidelines on edible oil intake, the country would project toward a production surplus by 2030 rather than a widening deficit. The PM’s economic concern and the medical recommendations point in precisely the same direction.
The Health Evidence
Medical literature is consistent on the core concern. A peer-reviewed comparative review in Nutrition Research Reviews (Cambridge, 2010) linked high saturated fat intake to obesity, insulin resistance, metabolic syndrome, stroke, and myocardial infarction. Monounsaturated and polyunsaturated fatty acids — found in mustard, groundnut, sesame, and sunflower oils — are associated with lower LDL cholesterol. Saturated fatty acids, dominant in palm oil, elevate LDL and increase cardiovascular risk.
A systematic review and meta-analysis in the BMJ (de Souza et al., 2015, PMID 26268692) found saturated and trans-fat intake associated with increased all-cause mortality, cardiovascular disease, and type 2 diabetes. A 2018 PLOS ONE systematic review of 25 studies found palm oil’s saturated fat content raises LDL cholesterol comparably to partially hydrogenated fats. The WHO’s July 2023 guidelines stated that high saturated fat intake “is correlated with increased risk of cardiovascular diseases.”
A further risk specific to Indian practice is the reuse of cooking oil across multiple sessions — common for reasons of cost in households and street food settings alike. A 2023 peer-reviewed narrative review (Soundararajan et al., PubMed PMID 37877148) found that repeated heating produces trans fats through lipid per oxidation, significantly elevating cardiovascular risk. This practice is most prevalent precisely where fried street food consumption is highest.
India's per capita edible oil consumption has nearly tripled
in 25 years to 23.5 kg — almost double the ICMR ceiling
of 12 kg. The peer-reviewed literature consistently links this level of saturated fat intake to cardiovascular disease,
type 2 diabetes, and fatty liver disease.
What Evidence Says Can Be Done
Shift to Indigenous Oils
The most direct dietary intervention supported by the literature is substituting refined palm oil with oils whose fatty acid profiles carry lower cardiovascular risk. A 2018 peer-reviewed study by Dorni et al. (Food Chemistry, DOI: 10.1016/j.foodchem.2017.05.072) found that mustard, groundnut, and sesame oils — all grown domestically in India — carry substantially higher proportions of MUFAs and PUFAs relative to saturated fats compared to refined palm oil. The ICMR recommends rotation between oil types for this reason. A shift in consumption would simultaneously improve public health and reduce import dependence on a single commodity.
What Tradition Knew and Science Has Confirmed
What Tradition Knew
Farm labourers across rural India still practice it without thinking about it: up at dawn, out to the fields on empty stomachs, working hard through the morning hours, returning in the afternoon to bathe, offer prayers, and eat their first proper meal. No nutritional guidelines consulted. They simply follow what the body tells them, and the body — given the chance to speak — tells the truth.
The very word jalpaan — the colloquial term for breakfast across many parts of India — originally meant precisely this: take water. Nothing more. In Gurukul times, teachers taught and students learned through the morning hours without eating. A Vedic text instructs the student, upon admission to study: “Take water and do thy work.” Water in the morning. Work. Then food. Somewhere in the passage of decades, the water became parathas, the parathas multiplied and swam in ghee, the ancient wisdom was buried — and most people today have never heard it existed.
Dr. Dewey’s Clinical Rediscovery
Dr. Edward Hooker Dewey, a 19th-century American physician, developed what he called the “No Breakfast Plan” after discovering through personal experience and clinical practice that abstaining from morning eating resolved a remarkable range of chronic ailments.
His foundational insight was that sleep is not a hunger-producing process — the morning appetite most people experience is not a genuine physiological signal but a conditioned response, habit dressed up as hunger. But what is striking is that Dewey was not discovering something new. He was rediscovering something India had always known.
What Peer-Reviewed Science Now Confirms
Dewey’s clinical intuitions, and India’s traditional practice, have since found their scientific grounding. A 2024 systematic review and meta-analysis in Nutrients (PMC11566317) analysed 11 studies on intermittent fasting and metabolic syndrome, finding significant improvements in body weight (mean reduction 3.59 kg), BMI, cholesterol, blood pressure, and glucose. A 2022 Nutrients review (PMC8839325) found time-restricted feeding — limiting intake to a defined daily eating window — induces fatty acid metabolism and produces favourable metabolic effects.
A 2023 randomized trial in Cell Reports Medicine found early time-restricted eating improved 24-hour blood glucose, glycaemic variability, and insulin sensitivity. A secondary analysis in Obesity (PMC9877132, 2023) found that adherence to an early 8-hour eating window (07:00 to 15:00) produced significantly greater improvements in body weight, body fat, insulin resistance, and blood glucose compared to controls.
The nuance matters: a 2025 Frontiers in Nutrition review cautioned that observational studies associate complete breakfast skipping with increased cardiovascular and type 2 diabetes risks. The evidence-supported approach is an earlier eating window — consuming earlier in the day, less late — not simply skipping morning food and compensating at night.
For Indian households, the practical implication is a lighter, less oil-intensive morning intake, with the principal caloric load at midday, directly reducing the fried breakfast foods that drive a disproportionate share of daily oil consumption.
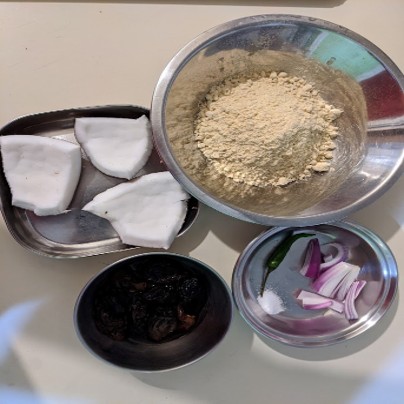
The complete raw morning larder: sattu flour, fresh coconut, dried fruit, onion and green chilli. Everything here is shelf-stable, inexpensive, available in every corner of India, and requires no cooking. This is not a health food store arrangement. It is what Indian kitchens have always had — rediscovered.
Raw Morning Alternatives: Zero Oil, Documented Nutrition
Replacing oil-dependent cooked breakfasts with raw alternatives is supported by the nutritional properties of the foods themselves. Sprouted legumes undergo enzymatic changes during germination that increase protein bioavailability and reduce anti-nutritional factors, as documented in food science literature.
Sattu — roasted gram flour — carries approximately 20 to 25 grams of protein per 100 grams, a low glycaemic index, and high fibre, making it among the most cost-effective plant protein sources in India. Fresh seasonal fruit delivers vitamins, antioxidants, and fibre with no oil and no LPG. Scaled across millions of households, a shift toward raw morning intake directly reduces both daily oil consumption and the fuel burned to produce a cooked morning meal — a tangible response to the PM’s twin concerns.

The raw morning alternative: sprouted moong and chana prepared overnight, with fresh vegetables requiring no flame, no oil, and no cooking whatsoever. Nutritionally dense, digestively light, and ready before the alarm has fully faded.
Stop Reusing Oil
The evidence on repeated heating is unambiguous. Discarding rather than reusing cooking oil directly reduces trans fat exposure and lipid peroxidation products documented in the health literature. This requires no equipment, no expenditure, and no change in cuisine — only a change in kitchen practice. It is the lowest-cost intervention available and carries the clearest evidence base.
Need of a Framework
The PM’s call to reduce cooking oil consumption is economically rational and medically supported. India has been importing the majority of its edible oil for three decades, paying a bill that has grown 15-fold, feeding a consumption culture that has outrun both domestic production capacity and the recommendations of its own medical authorities. The solutions exist in the agricultural policy literature, in the nutritional science, and in the food safety research reviewed above.
What has been lacking is the translation of an appeal into a framework — one that tells citizens not just what to reduce, but what to replace it with, grounded in evidence that makes the case for permanence rather than crisis compliance. Ancient Indian tradition, a 19th-century American physician, and multiple modern randomised controlled trials all point in the same direction. The PM has identified the right problem. The history, economics, and science reviewed here suggest the right response is considerably more detailed — and more durable — than a speech.
Key Sources and References
1. SEA: Annual edible oil import data, 2023-24 and 2024-25. Business Standard, November 2024 and November 2025.
2. NITI Aayog: Pathways and Strategies for Accelerating Growth in Edible Oils Towards Atmanirbharta. August 2024. PIB PRID 2049737.
3. National Mission on Edible Oils – background data. PIB PRID 2200287.
4. ICMR-NIN: Recommended dietary guidelines; 12 kg/capita/year edible oil ceiling. WHO ceiling: 13 kg/capita/year.
5. WHO: Guidelines on saturated and trans-fatty acid intake, July 2023. Rapid review on palm oil, February 2024 (ISBN 9789240088344).
6. de Souza RJ et al.: Saturated/trans fats and all-cause mortality, CVD, type 2 diabetes. BMJ 2015;351:h3978. PMID 26268692.
7. Soundararajan P et al.: Repeatedly heated edible oils and cardiovascular disease. Bentham Science, 2023. PMID 37877148.
8. Ismail SR et al.: Palm oil and cardiovascular disease risk. PLOS ONE, 2018. DOI: 10.1371/journal.pone.0193533.
9. Dorni C et al.: Fatty acid profile of edible oils consumed in India. Food Chemistry 2018;238:9-15. DOI: 10.1016/j.foodchem.2017.05.072.
10. Lichtenstein AH et al.: Palm oil vs trans fats. Tufts/USDA Human Nutrition Research Center, 2006.
11. Dewey EH: The No-Breakfast Plan and the Fasting-Cure. 1900. Published by the Health-Culture Company, Passaic, New Jersey.
12. Intermittent fasting and metabolic syndrome: systematic review and meta-analysis. Nutrients, 2024. PMC11566317.
13. Time-restricted feeding and metabolic health. Nutrients, 2022. PMC8839325.
14. Dawson et al.: Early time-restricted eating and cardiometabolic health. Cell Reports Medicine, 2023.
15. Early TRE (07:00-15:00) and metabolic improvements. Obesity, 2023. PMC9877132.
16. Intermittent fasting and cardiovascular risk. Frontiers in Nutrition, 2025. DOI: 10.3389/fnut.2025.1524125.
17. Business Standard: Every Indian now consumes 24 kg edible oil a year. April 21, 2025.
18. NMEO-OS approved October 2024. Budget Rs 10,103 crore, 2024-25 to 2030-31.
19. Historical sources on samosa: Amir Khusro (c.1300 CE); Ibn Battuta (14th century); Nimatnama-i-Nasiruddin-Shahi (15th century); Ain-e-Akbari (16th century).
Pics Courtesy : Bhuwan Mohan Prasad

Bhuwan Mohan Prasad
An alumnus of Indian Institute of Technology Kanpur and University of Toronto, Bhuwan Mohan Prasad combines his professional work as an engineering consultant with his passion for independent writing. His writing spans political policy, the environment, public health, and energy.


{kind=link}